Opioids and Other Common Substances: What You Need to Know
Abstract
This fact sheet focuses on opioids, a highly addictive class of substance with a high risk of unintentional overdose death. We review how opioid overdoses can be temporarily reversed with naloxone (Dhalla, et al., 2009; Straus, et al., 2013) and some important resources.
Opioids and the Brain
Opioids are a class of substances that include prescription pain medications (e.g., oxycodone, hydrocodone, and codeine) as well as the illicit drug heroin (National Institute on Drug Abuse [NIDA], 2018). Heroin and prescription pain medications are addictive, have the same chemical structure, and perform similar neurological actions in the human body (NIDA, 2018). Opioids are a Central Nervous System (CNS) depressant that slow the signaling in the CNS and provide a reduced sensation of pain (Stoeber, et al., 2018). Opioids work by attaching to the opioid receptors (“ports” that send and receive signals) in the brain, which are responsible for sensing pain and preventing pain signals throughout the body (Huxtable, et al., 2011; Stoeber, et al., 2018; Lintzeris & Nielsen, 2010). Opioids are one of the most commonly used medicines for acute pain management due to their effectiveness and ability to attach to the receptors so effectively (Huxtable, et al., 2011; Stoeber, et al., 2018).
Opioid Overdose
As mentioned above, the use of opioids, especially in combination with other CNS depressants (e.g., alcohol, benzodiazepines), causes slowing or dulling of the CNS. As the body’s critical functions slow, they can reach a dangerous level of inactivity or stop all together, resulting in an overdose (i.e., a toxic amount of a substance that overwhelms the body and can result in death; Steynor & Macduff, 2015; Stoeber, et al., 2018). Knowing the signs and symptoms of an opioid overdose could save a life. If you or someone you love is using opioids (i.e., prescription pain medication or heroin), it is important to be aware of the signs and symptoms of an opioid overdose and know how to administer naloxone quickly during an emergency (Green, et al., 2008).
| Common Substances Used with Opioids That Increase Risk of Overdose |
|
Benzodiazepines and Opioids |
| Alcohol and Opioids Alcohol is one of the riskiest substances that can be taken with opioids, since alcohol and opioids both depress the CNS resulting in slowed signaling and breathing (Gudin, et al., 2015). Research has found that alcohol is used with opioids more frequently than any other substance (Hickman, et al., 2008; Larance, et al., 2016). The most dangerous consequence of consuming alcohol with opioids is alcohol’s ability to cause “slow-acting” opioids to rapidly release their chemicals and increase their chemical actions in the body unintentionally (Gudin, et al., 2015). |
What to do in an Overdose Emergency
In an overdose situation, always call for emergency medical services (EMS) help first, then administer naloxone (Narcan ©) to provide a temporary overdose reversal and prevent overdose death until EMS arrives (Rando, et al., 2015). Remember the acronym CCAPSS (Call 9-1-1, Check Circulation, Airway, Pupils, Slurred Speech, and trouble Staying Awake) if you find yourself in a possible overdose situation (Schiller, 2019):
CALL 9-1-1 Immediately
Check circulation: "Do they have a pulse?"
Airway: "Are they able to breathe on their own? Are their lips blue or pale?"
Pupils: "Do they have pinpoint, or very small pupils?"
Slurred Speech: "Are they able to talk without severe slurring or mumbling?"
Staying Awake: “Do they seem to have trouble staying awake? Are they unconscious or unresponsive?”
If the person has difficulties in any of the above areas, they may be experiencing an opioid overdose. If you have naloxone on hand it would be appropriate to administer it.
Naloxone
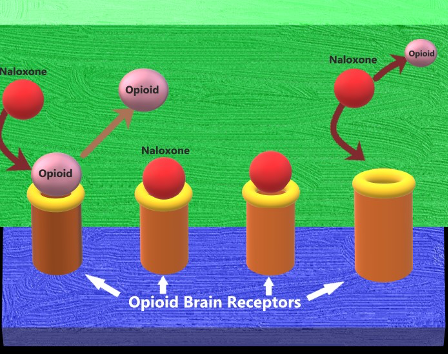
When opioids enter the brain, they act like a “key” and insert into specific opioid receptors, similar to a “lock” (Straus, et al., 2013). Naloxone has the potential to “knock” opioids off the brain’s opioid receptors. However, this only works for a short duration (approximately 30-90 minutes) before the opioids will re-attach to the brain’s receptors. In some cases where there are high levels of opioids present, a person may overdose multiple times or an overdose may require multiple doses of naloxone to reverse the overdose effects (Straus, et al., 2013; Lynn & Galinkin, 2017). Figure 1 shows how naloxone works on the brain’s opioid receptors to reverse an overdose.
Figure 1. Naloxone removes opioids from the brain receptor and attaches itself, reversing the effects of opioid overdose temporarily (e.g., Straus, et al., 2013).
What Else Should I Know?
In 2016, Utah passed the “Opiate Overdose Response Act” which allows pharmacists to dispense naloxone by the use of a “Standing Order” to anyone, without needing a prescription (Balough, et al. 2019; *some restrictions apply). Additionally, the “Good Samaritan Law” allows bystanders to report an overdose and provides some protections against prosecution in order to save a life (Balough, et al. 2019; *some restrictions apply). Please see Table 1 for a brief list of where to find more information.
Table 1. Opioid, Naloxone, and Emergency Resources and Websites
| General Utah Resources | Naloxone Websites | Emergency Numbers | Therapy Locator Websites |
|---|---|---|---|
| 211utah.org | Naloxone.org | 911 (EMS & Police) | Utahaddictioncenters.com |
| Opidemic.org | Utahnaloxone.org "Free Naloxone rescue kits available" |
1-800-273-8255 (Suicide Hotline) |
Intermountainhealthcare.org |
| Health.utah.gov. | Naloxoneforall.org | 1-800-222-1222 (Poison Control) |
Findtreatment.samhsa.gove |
| Utahsuicideprevention.org |
Note. All of the resources provided are for educational purposes and USU does not specifically endorse their services. Cognitive behavioral and other cognitive resources are intended to provide information, not to treat chronic pain or other mental health concerns. USU does not control the websites or books referenced above.
Always consult your medical provider when considering seeking treatment or management of a medical condition and/or medications.
Learn More:
In its programs and activities, Utah State University does not discriminate based on race, color, religion, sex, national origin, age, genetic information, sexual orientation or gender identity/expression, disability, status as a protected veteran, or any other status protected by University policy or local, state, or federal law. The following individuals have been designated to handle inquiries regarding non-discrimination policies: Executive Director of the Office of Equity, Alison Adams-Perlac, alison.adams-perlac@usu.edu, Title IX Coordinator, Hilary Renshaw, hilary.renshaw@usu.edu, Old Main Rm. 161, 435-797-1266. For further information on notice of non-discrimination: U.S. Department of Education, Office for Civil Rights, 303-844-5695, OCR.Denver@ed.gov. Issued in furtherance of Cooperative Extension work, acts of May 8 and June 30, 1914, in cooperation with the U.S. Department of Agriculture, Kenneth L. White, Vice President for Extension and Agriculture, Utah State University.
References
- Balough, M., Nwankpa, S., & Unni, E. (2019). Readiness of Pharmacists Based in Utah About Pain Management and Opioid Dispensing. Pharmacy, 7(1), 11. doi: 10.3390/pharmacy7010011
- Dhalla, I. A., Mamdani, M. M., Sivilotti, M. L., Kopp, A., Qureshi, O., & Juurlink, D. N. (2009). Prescribing of opioid analgesics and related mortality before and after the introduction of long-acting oxycodone. Canadian Medical Association Journal, 181(12), 891–896. doi: 10.1503/cmaj.090784
- Gomes, T., Mamdani, M. M., Dhalla, I. A., Paterson, J. M., & Juurlink, D. N. (2011). Opioid Dose and Drug-Related Mortality in Patients With Nonmalignant Pain. Archives of Internal Medicine, 171(7). doi: 10.1001/archinternmed.2011.117
- Green, T. C., Heimer, R., & Grau, L. E. (2008). Distinguishing signs of opioid overdose and indication for naloxone: an evaluation of six overdose training and naloxone distribution programs in the United States. Addiction, 103(6), 979–989. doi: 10.1111/j.1360-0443.2008.02182.x
- Gudin, J. A., Mogali, S. D., Jones, J. D., & Comer, S. undefined. (n.d.). Risks, Management, and Monitoring of Combination Opioid, Benzodiazepines, and/or Alcohol Use. Clinical Focus: ADHD, Psychiatric Disorders, and Pain Management, 125(4), 115–130. doi: doi.org/10.3810/pgm.2013.07.2684
- Hickman, M., Lingford-Hughes, A., Bailey, C., Macleod, J., Nutt, D., & Henderson, G. (2008). Does alcohol increase the risk of overdose death: the need for a translational approach. Addiction, 103(7), 1060–1062. doi: 10.1111/j.1360-0443.2008.02134.x
- Huxtable, C. A., Roberts, L. J., Somogyi, A. A., & Macintyre, P. E. (2011). Acute Pain Management in Opioid-Tolerant Patients: A Growing Challenge. Anaesthesia and Intensive Care, 39(5), 804–823. doi: 10.1177/0310057x1103900505
- Jones, C. M., Mack, K. A., & Paulozzi, L. J. (2013). Pharmaceutical Overdose Deaths, United States, 2010. Jama, 309(7), 657. doi: 10.1001/jama.2013.272
- Jones, C. M., & Mcaninch, J. K. (2015). Emergency Department Visits and Overdose Deaths From Combined Use of Opioids and Benzodiazepines. American Journal of Preventive Medicine, 49(4), 493–501. doi: 10.1016/j.amepre.2015.03.040
- Kameg, B. (2019). Shifting the Paradigm for Opioid Use Disorder: Changing the Language. The Journal for Nurse Practitioners, 15(10), 757–759. doi: 10.1016/j.nurpra.2019.08.020
- Larance, B., Campbell, G., Peacock, A., Nielsen, S., Bruno, R., Hall, W., … Degenhardt, L. (2016). Pain, alcohol use disorders and risky patterns of drinking among people with chronic non-cancer pain receiving long-term opioid therapy. Drug and Alcohol Dependence, 162, 79–87. doi: 10.1016/j.drugalcdep.2016.02.048
- Lintzeris, N., & Nielsen, S. (2010). Benzodiazepines, Methadone and Buprenorphine: Interactions and Clinical Management. American Journal on Addictions, 19(1), 59–72. doi: 10.1111/j.1521-0391.2009.00007.x
- Lynn, R. R., & Galinkin, J. (2017). Naloxone dosage for opioid reversal: current evidence and clinical implications. Therapeutic Advances in Drug Safety, 9(1), 63–88. doi: 10.1177/2042098617744161
- Marel, C., Sunderland, M., Mills, K. L., Slade, T., Teesson, M., & Chapman, C. (2019). Conditional probabilities of substance use disorders and associated risk factors: Progression from first use to use disorder on alcohol, cannabis, stimulants, sedatives and opioids. Drug and Alcohol Dependence, 194, 136–142. doi: 10.1016/j.drugalcdep.2018.10.010
- National Institute on Drug Abuse. (2018). Opioids. Retrieved April 9, 2020, from https://www.drugabuse.gov/drugs-abuse/opioids
- Rando, J., Broering, D., Olson, J. E., Marco, C., & Evans, S. B. (2015). Intranasal naloxone administration by police first responders is associated with decreased opioid overdose deaths. The American Journal of Emergency Medicine, 33(9), 1201–1204. doi: 10.1016/j.ajem.2015.05.022
- Schiller, E. Y. (2019, December 27). Opioid Overdose. Retrieved April 9, 2020, from https://www.ncbi.nlm.nih.gov/books/NBK470415/
- Stoeber, M., Jullie, D., Laeremans, T., Steyaert, J., Schiller, P. W., Manglik, A., & Zastrow, M. V. (2018). A genetically encoded biosensor reveals location bias of opioid drug action. Neuron, 98(5), 963–976. doi: 10.1101/254490
- Straus, M., Ghitza, U., & Tai, B. (2013). Preventing deaths from rising opioid overdose in the US – the promise of naloxone antidote in community-based naloxone take-home programs. Substance Abuse and Rehabilitation, 65. doi: 10.2147/sar.s47463
Authors
Justin R. Sacco, Health & Wellness Intern, B.S, NREMT; Ashley Yaugher, Ph.D.; Tim Keady, M.S., CHES; Kandice Atismé, MHA, MPH, CPH

Ashley Yaugher
Professional Practice Extension Associate Professor | Health and Wellness | HEART Initiative | Carbon & Emery Counties

Timothy Keady
Professional Practice Extension Assistant Professor | Health and Wellness | HEART Initiative

Kandice Atismé
Professional Practice Extension Assistant Professor | Health and Wellness | HEART Initiative | Davis and Weber Counties
Related Research

Anxiety and Depression: Can Diet Help?
In November 1944, Dr. AncelKeys and Dr. Josef Brozek, faculty at the University of Minnesota, conducted a study on the effects of starvation, known as the Minnesota Starvation Study (Baker & Keramidas, 2013). Through this study, it was observed that a lac

Benefits of Acceptance and Commitment Therapy (ACT) for Chronic Pain
According to the National Institute of Neurological Disorders and Stroke, pain is your body signaling that you have been, are, or are expecting to be injured or ill (NINDS, 2024). Pain is an unpleasant experience that motivates us to care for our bodies a

Cognitive Behavioral Therapies for the Management of Chronic Pain
Chronic pain is pain that lasts longer than six months and may continue even after illnesses or injuries have healed (Cleveland Clinic, 2017). Pain signals in the nervous system can remain active for several years if they are altered in the spinal cord, b

Diet, Nutrition, and Substance Use Disorder
Consuming a healthy diet can benefit everyone—especially individuals with substance use disorder (SUD), a disorder that occurs when frequent use of drugs or alcohol causes impairment, health issues, and difficulties with managing daily responsibilities (S

Evidence-Based Alternative Pain Management Techniques for Chronic Pain Relief
Pain is one way our bodies let us know that something is wrong. It alerts us if we have been injured, or if our bodies need care. Most pain is short-lived or “acute,” and subsides with minimal effort—but pain that lasts longer or doesn’t go away as quickl
Evidence-Based Pain Management Techniques for Chronic Pain Relief
Pain is one way our bodies let us know that something is wrong. It alerts us if we have been injured, or if our bodies need care. Most pain is short-lived or “acute,” and subsides with minimal effort—but pain that lasts longer or doesn’t go away as quickl

Exercise Tips for Chronic Pain Management
Chronic pain is a term used to describe pain that persists for longer than the expected time frame of healing. Patients with chronic pain commonly experience collateral effects to their primary condition. These include depression, sleep disturbance, fatig

Exercise and Chronic Pain
Chronic pain is perhaps the most pervasive medical issue in the United States. The long-term impacts of chronic pain often cause individuals to reduce or eliminate physical activity.

Fact Sheet for Parents: What You Need to Know About Adderall
This fact sheet educates parents about Adderall, its legitimate uses for treating ADHD and narcolepsy, and the dangers of misuse, including addiction, serious health risks, and exposure to counterfeit pills. It also provides practical advice on talking to

Fact Sheet for Parents: What to Know About ZYN Nicotine Pouches
This Utah State University Extension fact sheet informs parents about ZYN nicotine pouches, a smokeless, tobacco-free product that is discreet and highly addictive, making it popular among teens. It outlines health risks, warning signs of use, and how to

Fact Sheet: Fentanyl
This fact sheet provides an overview of fentanyl, a potent synthetic opioid used for pain management but increasingly found in illicit drugs, leading to a high risk of overdose. It explains the effects of opioids on the body, the dangers of fentanyl conta

Fact Sheet: Ketamine
Ketamine is a general anesthetic with pain-relieving properties that has gained attention for its potential antidepressant effects, though it also carries risks of psychological dependence and recreational misuse. While medically approved for anesthesia a

Fact Sheet: Methamphetamine
Methamphetamine is a highly addictive stimulant that dramatically increases dopamine levels, leading to intense euphoria, rapid dependence, and severe health risks, including heart problems, psychosis, and death. Misuse can result in dangerous side effect

First Responder Mental Health
Communities spend thousands of dollars on first responders to protect them physically: body armor for law enforcement officers, heat resistant gear for firefighters, gloves and reflective clothing for Emergency Medical Services (EMS) personnel. Supporting

Mindfulness for Chronic Pain Management
“ Mindfulness is ‘paying attention in a particular way: on purpose, in the present, and non judgmentally.’ ”

Naloxone: A Lifesaving Tool Against Opioid Overdose
Naloxone, commonly known by the brand name Narcan, is a safe and effective medication that can temporarily reverse the effects of an opioid overdose, potentially saving lives. It is available over the counter and protected under Utah’s Good Samaritan Law,

Neonatal Abstinence Syndrome (NAS): What You Need to Know
This fact sheet will talk about why and what to do, with recommendations for safe treatment and support during pregnancy.

Online Etiquette Guidelines
Below is a list of guidelines and general rules of thumb that, although are not mandatory, can increase communication quality in online platforms. They can be followed when presenting or conducting an online meeting with business

Pregnancy and Substance Use
This fact sheet will cover (1) the consequences of substance use and (2) the current recommendations for substance use during pregnancy.

Public Health Violence Prevention: Supporting Law Enforcement
The integrated biological-psychological-social model of health recognizes the complexity in the ways individuals are influenced by their situations, with violence as the unfortunate result of the wrong mix of circumstances. The public health approach to v

Reducing Stigma Towards Opioid Use Disorder Treatment
To better identify, understand, and eliminate stigma, this fact sheet discusses how stigma against treatment hinders recovery, evidence-based treatments for OUD, and strategies to combat OUD treatment stigma.

Staying Safe When Taking Prescription Opioids
This fact sheet from Utah State University Extension offers practical guidance on safely using prescription opioids. It explains how opioids work, the risks of dependence and overdose, and provides evidence-based strategies for pain management and harm re

Stigma and Mothers Using Opioids
Parenting and pregnancy in the context of substance use is a complicated topic. It is recognized as an important concern for child welfare (Chandler et. al, 2013). Many public health officials, social workers, policy makers, and community members want to

Substance Use Disorder Stigma: What it is and How You Can Prevent it
Stigma is an attitude, discrimination, or prejudice directed towards an individual or a group and can prevent a person from seeking out proper care, support, and treatment (Angermeyer & Dietrich, 2006).

Substance Use Disorders and Youth: How Parents and Communities can be Involved
This factsheet examines the effects of substance use on brain development in youth, the impact of Adverse Childhood Experiences (ACEs) on youth substance use, and interventions parents and community members can use to reduce their children’s risk.

Understanding the Teen Brain and Building Strong Relationships: A Foundation for Supporting Healthy Decisions
Understanding the complexities of the teen brain helps caregivers foster stronger relationships and support healthy decision-making. Discover strategies to build trust, encourage positive risk-taking, and navigate adolescence with compassion and connectio

Your Healthiest Year Yet: Practical Tips for Mental and Physical Well-Being
Prioritizing mental and physical wellness can lead to lasting improvements in overall health and daily life. By incorporating small, evidence-based habits—like mindfulness, regular exercise, and healthy eating—you can create a balanced and fulfilling year

Youth Treatment for a Substance Use Disorder and Common Barriers
This factsheet reviews youth substance use treatment, barriers that they face, prevention interventions, and resources for parents and community members.

Opioids and Other Common Substances: What You Need to Know
This fact sheet focuses on opioids, a highly addictive class of substance with a high risk of unintentional overdose death. We review how opioid overdoses can be temporarily reversed with naloxone (Dhalla, et al., 2009; Straus, et al., 2013) and some impo

Reducing Stigma Toward Medication-Assisted Treatment
Recovery and relationships can seem difficult on their own, while maintaining a healthy relationship during the recovery of one or both partners seem nearly impossible.

Recovery Relationships
You Are Not Alone Recovery and relationships can seem difficult on their own, while maintaining a healthy relationship during the recovery of one or both partners can seem nearly impossible. However, it is helpful to recognize that if you or y